Red Light Therapy for Breast Cancer Survivors: The Non-Hormonal Breakthrough for Vaginal Pain
Light Therapy After Breast Cancer: A Gentle New Option for Vaginal Pain and Sexual Dysfunction
You did the hard thing.
You faced breast cancer.
You went through surgery, chemo, radiation, hormone therapy - some or all of the above.
You showed up for every appointment. You followed every recommendation.
And now, when the world thinks you should just “feel grateful,” you’re dealing with something almost no one prepared you for:
· Vaginal burning and dryness.
· Pain or tearing with penetration.
· Loss of desire because your body just says “no”.
· Avoiding intimacy because it hurts - physically and emotionally.
Finally - some good news.
There is a growing body of research looking at a gentle, non‑hormonal therapy called photobiomodulation (PBM) - often described as “light therapy” - and the results for women like you are honestly impressive. Not perfect, not final, but very hopeful. (And it’s very likely that your providers likely don’t know ANYTHING about these tools). I know this becuase it hear it so often from the women I write protocols for.
This article walks you through one of the most exciting new studies in this area, and the growing research.

Order your pelvic light therapy wand and let’s work together to help you feel better - fast.
What is photobiomodulation?
Photobiomodulation (PBM) is a big word for a simple idea:
Using very gentle, low‑intensity light (usually red, near‑infrared, and sometimes blue) to help your cells heal and function better.
We’re not talking about hot surgical lasers, burning, or cutting. PBM uses light‑emitting diodes (LEDs) or low‑power lasers at carefully controlled doses that:
· Support cellular energy production (ATP)
· Improve blood flow
· Calm inflammation
· Support tissue repair and collagen remodeling
In the vaginal area, PBM has been studied for:
· Genitourinary syndrome of menopause (GSM).
· Vulvovaginal dryness and pain.
· Sexual dysfunction after cancer treatments.
· Chronic pelvic pain.
The core idea: help the tissue heal and function better without hormones, which is a huge deal when you’re on tamoxifen, aromatase inhibitors, or have a hormone‑sensitive cancer.
The latest (and most exciting study): light therapy for sexual pain on hormone therapy (June 2026)
A 2026 clinical study looked specifically at women who:
· Had a history of breast cancer.
· Were taking hormone therapy (like tamoxifen or aromatase inhibitors).
· Were experiencing severe vaginal pain and sexual dysfunction linked to that treatment.
These women weren’t just “a bit uncomfortable.” At baseline:
· Over 80% reported maximum pain (10 out of 10) with vaginal touch or penetration.
· Nearly 80% had absent or severely impaired sexual function.
Sex was pretty much off the table.
Who was in the study?
· 24 women agreed to receive PBM treatment.
· 8 additional women met the same criteria but declined PBM (mostly due to embarrassment) and were followed as a non‑treated comparison group.
What did the light treatment look like?
PBM was applied using a medical LED device designed for vaginal and vulvar tissues:
· 4 treatment sessions total.
· 1 session per week for 4 weeks.
· Each session included time using blue light and time using red light.
It followed a gentle, mucosa‑friendly dose, similar to what’s used in other vaginal red light therapy studies.
Impressive Findings
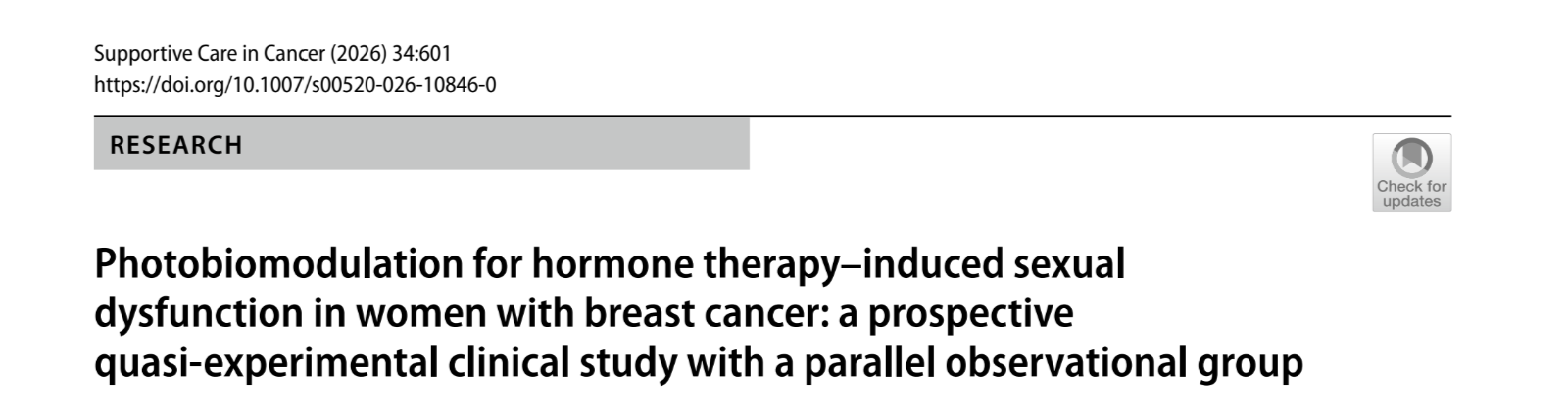
1. Pain: from “unbearable” to “almost gone”
At the start:
· 82.6% of women in the PBM group reported maximum vaginal pain (VAS = 10/10).
After only four PBM sessions:
· Average pain scores fell from about 9.5 to just over 1 (that number alone should make everyone involved in women’s intimate health sit up and take notice).
· About 79% of women reported complete absence of pain.
The women who did not receive PBM? Their pain stayed high. No meaningful change over the same time.
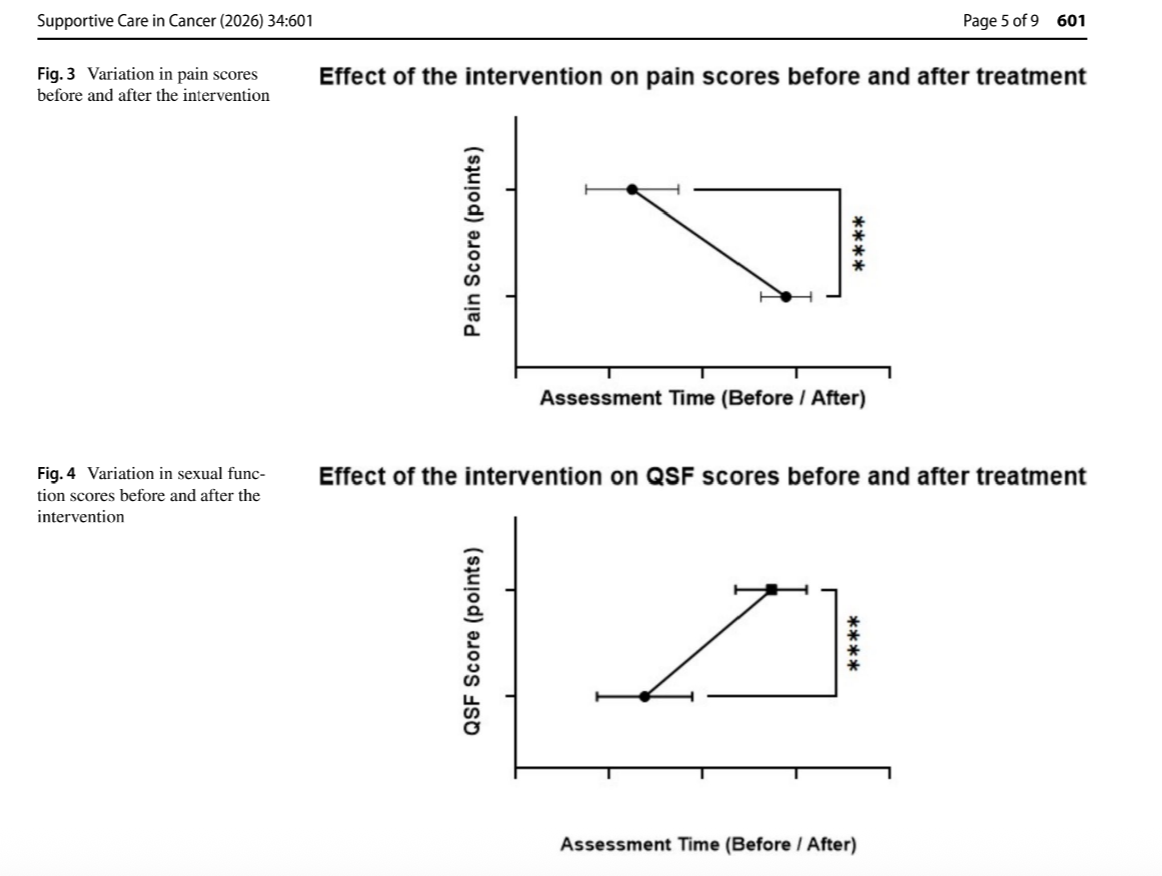
2. Sexual function: from “shut down” to “good or excellent”
Before PBM:
· Most women had absent or severely impaired sexual function - essentially, sex was out of the question.
After four sessions:
· Sexual function scores (on a 0–100 scale) jumped from about 23 to 87.
· 95.8% of women reported good to excellent sexual function after treatment.
The comparison group - women who declined PBM - stayed at zero sexual activity and zero improvement.
After 4 weeks of vaginal light therapy, almost 96% of women in this trial reported good to excellent sexual function.
3. Safety and tolerability
· There were no adverse events.
· A few women described a mild warming sensation inside their vagina during treatment but they didn’t need to stop. Some warming is expected as local circulation increases.
· This is consistent with other vaginal PBM devices that have reported excellent safety and high patient satisfaction in early studies.
For a population that often has very few non‑hormonal options, this combination of big symptom improvements + good tolerability is a big deal.
This isn’t the only red light therapy data we have for women’s sexual health.
This one trial isn’t happening in isolation. Other research is pointing in the same direction:
· A French cohort of women with vulvovaginal problems after cancer treatments (including hormone therapy) found that after at least 6 PBM sessions, about 72% of women felt “better” or “much better,” with a median improvement of 65% and no serious adverse events.
· A 2026 prospective study in genitourinary syndrome of menopause (GSM) used intravaginal 660‑nm PBM once weekly for 8 weeks. Vaginal health scores improved significantly, urinary symptoms eased, sexual function scores rose, and no adverse events were observed.
· A first‑in‑human safety study of a dedicated vaginal PBM probe (MILTA GYNECO) showed that the device was safe, well‑tolerated, and associated with improved pain and vaginal health, supporting future randomized trials.
Taken together, these studies show that PBM is emerging as a legitimate, non‑hormonal option for vulvovaginal pain and sexual problems - especially in women who’ve already been through cancer treatments.
A Note for Skeptics (And why it’s actually a good thing.)
If you’re a clinician - or you’ve talked to one - there may be some skepticism about PBM. That’s understandable.
You’ve seen plenty of over‑promised “fixes” for women’s intimate health.
And you are absolutely right to ask questions like:
· Where are the big randomized trials?
· How long do the benefits last?
· Are we sure this is safe in women with a history of cancer?
All fair questions.
Here’s what we can say right now:
· We do have multiple peer‑reviewed clinical studies (like the one you just read about) showing substantial improvements in pain and sexual function with vaginal PBM in post‑oncology and GSM populations.
· We do not yet have huge, multi‑center RCTs with hundreds of patients. Given how under‑funded women’s intimate health has been, that’s sadly not surprising.
· Early safety data, including in women after cancer, have been reassuring when PBM is used at appropriate doses and away from active tumor sites.
So this is not about abandoning healthy skepticism. It’s about updating it in light of emerging evidence.
Women are already looking for solutions. Let’s make sure they’re safe.
Here’s the reality:
Women who are living with “10 out of 10” pain, or who haven’t been able to have comfortable sex for years, are not waiting for perfect RCTs before they look for help.
They’re already:
· Searching online.
· Listening to podcasts.
· Joining Facebook groups and forums.
· Buying devices online - with zero guidance and often end up either under or overdosing (so they’re a lot less likely to see the same results the studies it and conclude red light therapy is a scam).
Not because they’re irresponsible. Because they’re desperate and under‑served.
So the question is not whether we recommend red light therapy to women.
But how do we help women find the safest, most evidence‑aligned options possible - rather than hyped‑up “cures” with no data behind them?
That’s where research like this matters.
· It shows what was actually used: wavelengths, timing, number of sessions.
· It documents real outcomes: how much pain decreased, how much sexual function improved, and whether anyone had adverse events.
· It gives both women and clinicians something concrete to talk about, rather than leaving them with marketing claims alone.
For women, that means:
· You can be curious and proactive.
· You can ask your team about PBM and share these studies.
· You can insist on options that are non‑hormonal yet grounded in real science, not just trends.
For clinicians, it means:
· You don’t have to instantly endorse every device.
· But you can distinguish between:
o Evidence‑based PBM approaches, and
o Random gadgets making big promises without data.
· You can help guide your patients toward safer, smart experimentation instead of leaving them totally on their own.
Why where you get your device matters
Because women are already looking for solutions, with or without their provider’s blessing - where and how they access light therapy becomes really important.
Buying a random “vaginal light gadget” off Amazon usually comes with:
· No real dosing guidance.
· No linkage to actual PBM studies.
· No help adjusting if symptoms change.
· No one to ask, “Is this normal?” or “Should I keep going?”
That’s how good intentions turn into frustration - or in some cases, unnecessary risk (especially when nerve damage is part of the picture).
One of the reasons I chose to make vetted devices available through my own work is to close that gap and make sure women aren’t doing this entirely alone.
When a woman purchases through my website, you don’t just get a device. You get:
· Ongoing support
o A real human to ask, “Is this the right mode?” or “What if my pain flares after a session?”
o Clear information about what the research shows - and what it doesn’t.
· Personalised protocol guidance
o Session structure and progression modeled on clinical studies (like the breast‑cancer PBM trial you’ve just learned about), then adapted to your specific situation: fertility, post‑oncology, GSM, postpartum, etc.
· Symptom tracking and interpretation
o Simple tools to track vaginal pain (VAS) and sexual function over time, so you can see whether it’s actually helping instead of guessing.
o A framework for deciding when to hold, adjust, or stop based on her body’s response - not just the marketing promises on a box.
· Evidence‑informed dosage instructions
o Clear starting timing, how to ramp up conservatively, and when enough is enough, grounded in published PBM parameters for vaginal tissues rather than generic “10 minutes a day for everyone.”
· Integration with your existing care
o Language and summaries she can share with your oncologist, gynecologist, or pelvic PT, so light therapy isn’t happening in a silo - they can weigh in, monitor, and feel part of the process.
Because the reality is:
Women will seek relief.
They will try things.
The choice is whether they do that in isolation, guided only by ads and anecdotes - or with support, structure, and science behind them.
The bottom line
· Yes, vaginal pain and sexual dysfunction after breast cancer and hormone therapy are common - and profoundly under‑treated.
· Yes, a growing number of studies show that (PBM) can significantly reduce pain and improve sexual function in this population, with good short‑term safety.
· No, this isn’t yet a fully standardized, guideline‑approved therapy with giant RCTs behind it.
· But it is a real, emerging, non‑hormonal option that deserves a place at the table - especially for women who have already been told “there’s not much else we can do.”
If you’ve been feeling unseen in this part of your recovery, know this:
Your pain is real.
Your sexuality is not a luxury.
And there are clinicians, researchers, and device designers actively working to bring safer, research‑aligned options - like PBM - into your hands.
Tracy
Additional Resources:
https://blog.tracydonegan.org/blog/best-red-light-pelvic-wand-for-women
https://blog.tracydonegan.org/blog/red-light-therapy-and-vulvar-lichen-sclerosus
https://blog.tracydonegan.org/blog/red-light-therapy-for-urinary-incontinence-and-menopause
1. https://pubmed.ncbi.nlm.nih.gov/42228167/
2. https://pubmed.ncbi.nlm.nih.gov/37183056/
3. https://pmc.ncbi.nlm.nih.gov/articles/PMC6648197/
4. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0351765
5. https://pmc.ncbi.nlm.nih.gov/articles/PMC6091542/
6. https://pubmed.ncbi.nlm.nih.gov/41404945/?fc=None&ff=20260104114207&v=2.18.0.post22+67771e2
7. https://www.liebertpub.com/doi/full/10.1089/whr.2021.0097
8. https://becarispublishing.com/doi/10.2217/cer-2021-0187
9. https://pubmed.ncbi.nlm.nih.gov/42329990/
10. https://www.sciencedirect.com/science/article/abs/pii/S0007455123001625
11. https://www5.bahiana.edu.br/index.php/medicine/article/view/1472
12. https://pmc.ncbi.nlm.nih.gov/articles/PMC8362505/
13. https://pubmed.ncbi.nlm.nih.gov/30406341/
14. https://repositorio.bahiana.edu.br/jspui/handle/bahiana/1628
16. https://pubmed.ncbi.nlm.nih.gov/20017385/
17. https://onlinelibrary.wiley.com/doi/10.1002/cam4.3582
18. https://pmc.ncbi.nlm.nih.gov/articles/PMC11853966/