Red Light Therapy and Vulvar Lichen Sclerosus
Updated June 2026
What is Vulvar Lichen Sclerosus?
If you’ve never heard of vulvar lichen sclerosus (VLS), consider yourself fortunate.
And if you have heard of it, or you're living with it, you know it’s so much more than a ‘skin condition.’
VLS is a chronic, inflammatory autoimmune condition that affects the vulva and sometimes even the skin around the anus. It’s often itchy, painful, and, honestly for some women completely life-altering. It can also result in fusion or adhesions that can occur when areas of the vulva, such as the labia minora (inner lips), stick to the labia majora (outer lips) and it can impact the clitoral hood. Often some of the earliest signs of LS are pale, shiny patches of the skin and an unrelenting itch.
It can cause burning, pain with intimacy and even tearing of the skin… as well as deep emotional distress. If you have been diagnosed with this condition I’m sorry you’re feeling so miserable - for too long, treatment options have been limited to steroid creams and crossing your fingers. VLS tends to show up most often early in life (before puberty) and later in life (after menopause). It’s less common during the reproductive years (teenagers through about mid-40s) so it seems likely there’s a hormonal aspect to it.
But here’s the good news - and you know I love bringing you good news.
Photobiomodulation (PBM), also known as low-level laser therapy (LLLT) or red light therapy is showing serious promise as a way for women to get natural relief for vulvar lichen sclerosus in a non-invasive way to help manage the symptoms of vulvar lichen sclerosus. The research is exciting, but as usual we need a LOT more focus on women's health, especially this debilitating condition.
(My recommended Red Light Products for women’s health - hand held laser for VLS

Image credit - Volodymyr Bushmelov - Solasta handheld laser for vulvar lichen sclerosus photobiomodulation therapy.
How is Lichen Sclerosus Treated?
There currently is no cure however there are treatments that can reduce the symptoms (see the end of my article for recent updates - June 2026).
Steroids are often a first line of reducing the inflammation, but they’re not recommended for long term use as they can thin the skin even further. For women who can’t tolerate steroids for LS immunomodulators may be suggested which are non-streroidal treatments but can cause a stinging sensation. Some providers use a combination approach of both. Note the name - immuneomodulator - a treatment that modulates the immune system…which brings us to another approach to modulating the immune system - red light therapy.
Red Light Therapy for Lichen Sclerosus
Red light therapy/photobiomodulation for lichen sclerosus uses red and near-infrared light to stimulate cellular within the tissues. We start at the tiniest common denominator - your cells, and when we give them more energy for healing and reducing inflammation the tissues of the vulva can heal. It's like giving your cells a little TLC to help them reduce inflammation, soothe pain, and start the repair process. This is NOT a CO2 laser - there is no burning, no cutting, no downtime - just gentle light on your bits for a few minutes a week for several weeks. The Solasta Handheld Laser can be used to reduce discomfort and improve collagen production in this sensitive area.

Solasta handheld laser for vulvar lichen sclerosus photobiomodulation therapy.
How Photobiomodulation (PBM) Targets VLS at the Source
Unlike traditional CO2 lasers that resurface skin through heat, PBM uses red and near-infrared light to "recharge" your cells. Think of it as cellular TLC. By increasing mitochondrial function within the epithelial cells, we:
Reduce inflammation and oxidative stress.
Decrease pain by calming TRPV channels.
Boost collagen to help with tissue elasticity and adhesions.
Blue Light: A New Player in the LS Light Therapy Toolkit?
While we often talk about Red and Near-Infrared light, there is a newer option gaining attention: Blue Light therapy. You might have heard of blue light for treating acne, but early clinical research shows it could have a special place in managing VLS symptoms, too.
Studies using medical-grade blue light have found that it can help reduce itching and pain, while also calming redness and helping those painful "fissures" (small skin tears) heal.
How Blue Light Works Differently
Think of Red light as the "deep healer" and Blue light as the "surface specialist."
Surface Relief: Blue light stays very superficial. It doesn't penetrate deep like infrared light; instead, it focuses its energy on the very top layers of your skin.
Targeting the Itch: Because much of the intense burning and itching of VLS is felt right on the surface, blue light can help calm that inflammation exactly where it’s happening.
The "Sweet Spot": Why More is Not Better
With blue light, there is a very important rule: A little goes a long way. In moderate doses, blue light is a "healing support." However, science shows that at very high doses, blue light (specifically in the 400 - 420 nm range) can actually flip and become an irritant, potentially damaging skin cells or collagen.
If you are experimenting with a device like the Fringe Wand - which includes a 415 nm blue light setting - safety is the priority and we’ll work together with very low conservative dosing to begin with.

Blue wavelenghts can be helpful for itching but not tissue atrophy and pain - that’s where red light excells.
The Denmark Study: Real Relief for Chronic Symptoms
A recent study followed 94 women who didn't find enough relief from steroid creams alone. After ten sessions of 808 nm low-level laser therapy, the results were life-changing:
Dramatic drop in pain levels.
Improved sleep and energy.
Significant boost in emotional well-being.
And the best part - no serious side effects.
Brazilian Pilot Study
We know that the "gold standard" for Lichen Sclerosus (VLS) has always been high-potency steroid creams. But if you’ve used them, you know they come with a catch. A fascinating pilot study out of Brazil recently put steroids head-to-head with red light therapy (Photobiomodulation), and the results give us a very clear picture of the Sprint vs. The Marathon in LS healing.
Here is the breakdown of what they found and why it matters for your treatment plan.
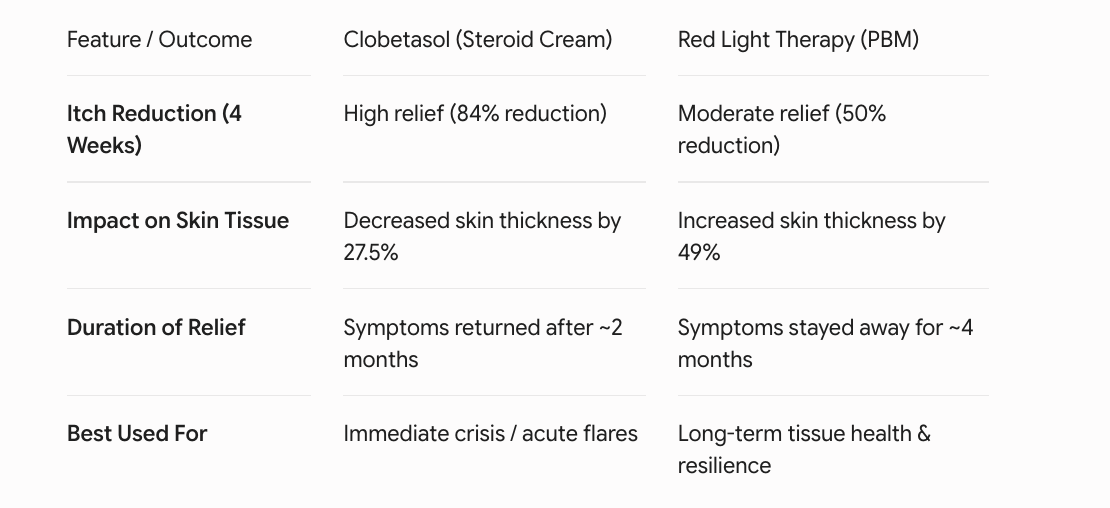
The Study: Steroids vs. Light
Researchers followed 20 women with confirmed VLS. They split them into two groups for a 4-week trial:
Group A (The Steroid Group): Used Clobetasol once a day.
Group B (The Light Group): Received red light therapy (PBM) laser just once a week.
The Results: A Tale of Two Timelines
1. The "Itch" Factor (The Sprint)
If you need immediate relief from a brutal flare-up, steroids are the fast lane.
Steroids: Reduced itching by 84%
Light Therapy: Reduced itching by 50%
Steroids are faster at calming that initial, maddening itch.
2. Skin Health (The Long Game)
This is where the study gets really interesting. LS already makes the skin thin and fragile, and we know that long-term steroid use can make that worse.
Steroids: Skin thickness decreased by 27.5%. The cream helped the itch, but it thinned the skin further.
Light Therapy: Skin thickness increased by 49%.
PBM actually helped rebuild and "plump up" the tissue, making the skin healthier and more resilient.
3. How long did the relief last?
The researchers checked back in several months after the treatments stopped to see when the symptoms returned.
Steroids: Symptoms started coming back after about 2 months.
Light Therapy: Symptoms stayed away for about 4 months.
Even though the light therapy took longer to get started, the relief lasted twice as long as the steroids.
What does this mean for you?
It’s not necessarily about choosing one or the other; it’s about using the right tool for the job and many women continue to use both while getting inflammation under control.
For a Crisis: If you are in a massive flare, steroids are excellent for putting out the fire quickly.
For Long-Term Health: If you want to stop the cycle of thinning skin and frequent relapses, Photobiomodulation (PBM) is the marathon runner. It supports the skin’s structure and keeps you in the clear for much longer.
This study was small, but it's quite heartening. It suggests that red light therapy is a powerful way to support or even reduce the need for steroids, giving your "bits" a chance to actually heal and thicken rather than just being "numbed" to the pain.
Beyond Steroids: Why Having More LS Treatment Options Matters
VLS can steal so much, confidence, comfort, sleep and intimacy. Having more tools like red light therapy in our healing toolkit means women aren’t stuck choosing between suffering or relying 100% on steroids (especially if steroids haven’t helped).
And you deserve options. You deserve to feel good in your body.
Period.

Red light therapy reduces inflammation and oxidative stress at the source by increasing mitochondrial functioning within the epithelial cells. Photobiomodulation increases anti-inflammatory cytokines and reduces pain through TRPV channels.
If you’re using my home laser you’ll receive a personalized protocol for you to replicate the most effective research protocols as closely as possible.
The JAK-STAT Pathway, JAK Inhibitors & Red Light Therapy: A New Frontier in Lichen Sclerosus Treatment (June 2026 update).
Why This Is Such a Big Deal? We Now Know the "On Switch" for LS Inflammation
For years, lichen sclerosus research was frustratingly vague about why the immune system keeps attacking vulvar skin. That has now changed. Recently a molecular ‘GPS’ that maps exactly which genes are active in which cells has identified a specific inflammatory signalling pathway that is consistently "switched on" in LS lesions: the IFN-γ / JAK-STAT pathway.
Dr. Andrew Goldstein, one of the world's leading vulvar lichen sclerosus specialists, has been a key voice in bringing this research into clinical focus. In his work, one signalling pathway was consistently elevated across almost all lesional samples: JAK/STAT - and critically, the sample with the least JAK/STAT activation had the least severe disease. This is fantastic news because it tells us precisely where to direct treatment.
What IS the JAK-STAT Pathway?
Think of the JAK-STAT pathway as a fire alarm system in your cells.
When your immune system detects a threat, it releases a cytokine called IFN-γ (interferon-gamma). IFN-γ is like someone pulling the fire alarm. That alarm signal travels to the surface of a skin cell (a keratinocyte), and binds to a receptor. This activates enzymes called JAK1 and JAK2 (Janus Kinases), the wiring between the alarm and the sprinklers. The JAK enzymes then activate STAT proteins, which travel to the cell's nucleus and switch on inflammatory genes.
In LS, this fire alarm is stuck in the ON position. Even when there's no new infection or injury, IFN-γ keeps signalling, JAK keeps firing, and STAT keeps activating genes that drive inflammation, cell stress, and the characteristic thinning and scarring of lichen sclerosus.
The latest research identifies keratinocytes (your skin cells) as the central players - they are both targets of IFN-γ signalling and senders of inflammatory alarm signals (called alarmins), creating a destructive feedback loop.
Enter the JAK Inhibitors: Ruxolitinib (Opzelura) and Others
Once you know the fire alarm is stuck, the solution becomes clearer: switch off the JAK-STAT pathway. That is exactly what a class of drugs called JAK inhibitors (jakinibs) do.
Ruxolitinib (brand name Opzelura as a topical 1.5% cream) is the most talked-about topical JAK inhibitor currently being studied for LS. It is already FDA-approved for atopic dermatitis and vitiligo.
When ruxolitinib is applied topically to the area affected, it blocks the JAK1 and JAK2 enzymes at the cell membrane receptor. Without functional JAK enzymes, IFN-γ cannot transmit its signal intracellularly. The STAT proteins cannot be activated, cannot travel to the nucleus, and cannot switch on inflammatory genes. The fire alarm gets disconnected at the wiring.
A 2025 systematic review confirmed that baricitinib and abrocitinib (oral JAK inhibitors) have the highest current evidence for genital LS, with significant reductions in pruritus, pain, and quality of life improvements. Topical ruxolitinib case reports in LS, including in children showed noticeable symptomatic improvement and significant improvement in skin lesions. A 2025 retrospective study of refractory LS identified JAK inhibitors as showing the most promise for steroid-resistant cases.
It is important to note this is an emerging evidence base, while single-arm trials are promising, large randomized controlled trials are still underway.
How Does Red Light Compare? Mechanism Side-by-Side
This is where it gets really interesting for women already using my Solasta laser for their LS. Red light therapy and JAK inhibitors are taking different but complementary routes to calm down the same inflammatory storm.
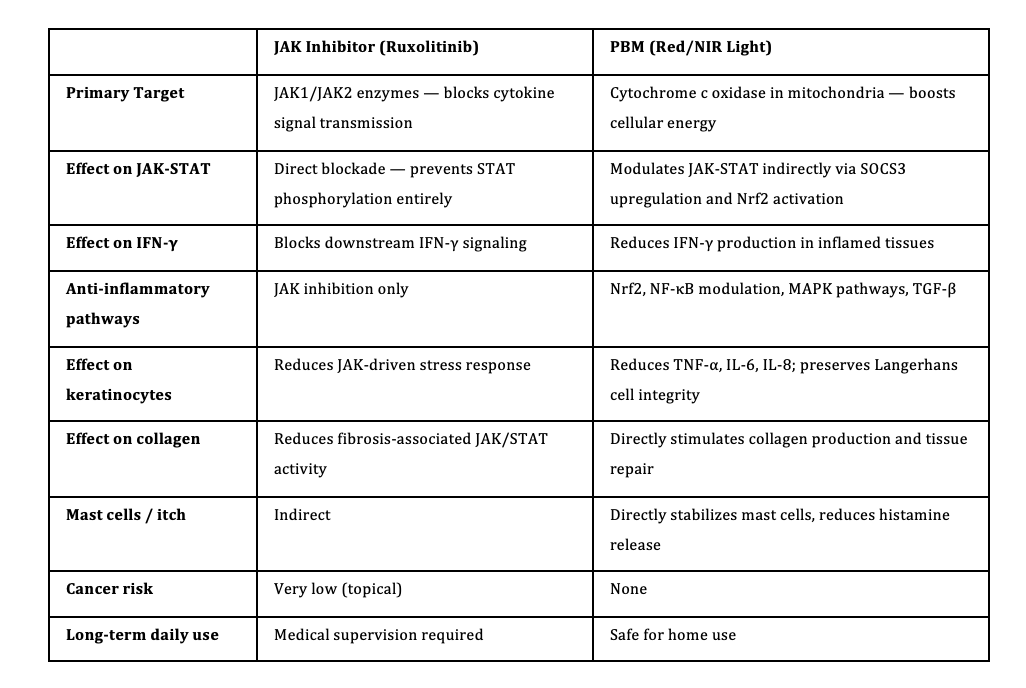
Are There Benefits to Combining Home Red Light Therapy Laser and JAK inhibitors?
At the time of writing (2026), as JAK hasn’t been approved yet for LS we don’t have studies specifically combining topical JAK inhibitors with photobiomodulation for lichen sclerosus, but the mechanistic case is strong. JAK inhibitors block the signal directly; Red light therapy modulates the pathway naturally, addresses oxidative stress, rebuilds collagen, and stabilizes mast cells. Together, they could target both the inflammation and the structural consequences of long-standing LS. Watch this space!
JAK Inhibitors for LS — What's Available Right Now
So we now know the JAK-STAT pathway is the "on switch" stuck in the wrong position in LS and JAK inhibitors can help turn it back off. The question everyone is asking: can I actually get my hands on it?
The short answer is: yes - but with a few important caveats.
The Topical Cream: Ruxolitinib (Opzelura)
The most exciting option for LS is a topical JAK inhibitor cream called ruxolitinib (brand name Opzelura, 1.5% cream). It's already in US specialty pharmacies, it just needs a prescription.
It's been FDA-approved since 2021 for eczema and since 2022 for vitiligo. In September 2025 it was expanded to children as young as 2. The catch? It is not yet FDA-approved specifically for lichen sclerosus. Any use for LS right now is off-label, completely legal and common in medicine, but it does mean you need a doctor paying attention to the latest LS research.
Think: a vulvodynia specialist, a vulvar disease dermatologist, or someone in Dr. Goldstein's circle. Your gynae/dermatologist may not be there yet and that's okay, but you may need to be your own advocate.
One more thing: pharmacy shortages as of mid-2026 mean Opzelura is primarily available through specialty pharmacies rather than your regular pharmacy.
Side Effects - The Reassuring Reality
In clinical trials, fewer people on Opzelura reported side effects than people on the placebo cream. In a real-world review tracking nearly 14,000 patient-years of use, there were no very few serious events.
Common: mild application site irritation (actually lower than placebo), cold-like symptoms.
Rare: shingles reactivation, folliculitis.
No skin thinning, no stretch marks - a meaningful difference from long-term clobetasol.
About the Black Box Warning: The cancer/infection warning on Opzelura's packaging was carried over from studies on oral JAK inhibitor pills in older rheumatoid arthritis patients - a very different picture from a cream applied to the vulva. The cream delivers only about 5% of the drug into the bloodstream. For LS patients managing an elevated SCC risk, the topical cream is unlikely to suppress the whole-body immune surveillance that protects you.
The Bottom Line
None of these are yet officially approved for LS, clinical trials are still underway. But they exist, are prescribable today, and specialists are already using them for women who haven't responded to clobetasol.
Cost: Unfortunately, Opzelura can cost from $700 - $900/month without insurance, though Incyte (the manufacturer) offers copay assistance.
The route in is through a specialist. Ask specifically about off-label ruxolitinib cream for lichen sclerosus. Bring the research. You deserve a doctor who will look at it with you.
And the big picture? PBM and JAK inhibitors are not either/or. The cream targets the broken alarm switch directly; Laser therapy works on the same pathway from a different angle while also rebuilding the tissue and calming the mast cells that drive that relentless itch. Used together, under specialist guidance, they may well be more powerful than either alone.
As always - more research please, and faster. Women deserve better options.
Your Questions Answered: JAK Inhibitors & LS
Q: How often do you apply the cream?
Opzelura is applied as a thin layer twice daily - morning and evening - directly to the affected external vulvar skin. It's not a "use it when things flare" cream - the twice-daily routine is what builds the anti-inflammatory effect over time. One practical note: wash your hands after applying (unless your hands are also being treated), and do not apply inside the vagina - external skin only.
Q: Can I use it at the same time as clobetasol?
Not layered on top of each other at the same time — but they work really well as a team. The approach specialists are exploring is: use clobetasol for acute flares (short bursts to get things under control quickly), then transition to Opzelura for maintenance in between. Think of clobetasol as the fire extinguisher and Opzelura as the fire prevention system. One meaningful advantage of Opzelura over long-term clobetasol: no skin thinning, no stretch marks - so it's a safer option for ongoing use on delicate vulvar tissue.
Q: How long do you use it for?
For eczema, the guidance is to use it until symptoms resolve, then stop and restart if needed. For LS, which is a chronic condition that doesn't "go away" this is more nuanced and still being worked out by specialists. Unlike a short course of antibiotics, women with LS should expect this to be an ongoing conversation with their doctor rather than a finite treatment. Regular monitoring (including regular vulvar skin checks given LS's associated SCC risk) remains essential.
Q: What happens when you stop?
JAK inhibitors manage the inflammation - they don't fix the underlying immune dysfunction that causes it. When oral JAK inhibitors have been stopped in LS trials, symptoms tend to return. This is one reason why red light therapy as a long-term complementary daily practice is so valuable - it works on tissue repair, mast cell stabilisation, and immune modulation at a level the cream can't address, and is safe to continue indefinitely alongside (or after) any pharmaceutical treatment.
Q: Can I use it alongside my red light therapy / PBM sessions?
Just like usising Clob - sensible practical advice would be: don't apply the cream immediately before a PBM session, as light can affect skin permeability. Either do your PBM session first and wait 60 minutes before applying, or use the cream at a different time of day from your light therapy.
Q: I'm pregnant or trying to conceive — can I use it?
No - ruxolitinib cream is not recommended during pregnancy. It falls into the "insufficient safety data" category, and some animal studies at high doses showed risk. This is a conversation to have with your specialist, don't stop any LS treatment without medical guidance.
Q: I'm not in the US — can I access this?
Availability varies significantly outside the US. In Canada, Opzelura is not currently reimbursed by public drug plans, making cost a major barrier. In the UK and Ireland, it has HCP approval for eczema but access for LS off-label use requires a specialist willing to prescribe it privately. In Australia, it is not yet widely available. If you are outside the US, your best route is through a vulvar disease specialist or dermatologist who follows international LS research, and being upfront about wanting to discuss emerging JAK inhibitor options.
Q: Is this a cure?
Honestly? No, not yet. What JAK inhibitors offer is a much more targeted way to manage LS than we've had before. Rather than broadly suppressing the immune system (like clobetasol does), they switch off the specific faulty pathway driving the damage. For women who have struggled with clobetasol resistance or the long-term effects of steroid use, that's a genuinely meaningful step forward. Combined with laser therapy for tissue repair and mast cell management and regular monitoring, we are getting closer to a management strategy that works with your body rather than just damping everything down.
The research is moving fast!
Frequently Asked Questions About Red Light Therapy for Lichen Sclerosus
These are the "hard truths" that often get missed in general red light therapy discussions. When it comes to a condition as specific and localized as Vulvar Lichen Sclerosus (VLS), the delivery of the light is just as important as the light itself.
Can you do red light therapy for lichen sclerosus at home?
Yes - but with a major caveat. Home treatment is only effective if you use a targeted, handheld device designed for close-contact or direct-skin use. Because VLS affects the delicate, recessed tissues of the vulva, generic wellness devices often fail to deliver the energy where it's actually needed. Home low level laser PBM is a fantastic way to maintain the results of any clinical treatments, but it requires the right tool and a consistent protocol.
Is PBM the same as a "laser" treatment?
This is where the terminology gets confusing.
Surgical/Ablative Lasers (like CO2 or MonaLisa Touch): These use heat to create "micro-injuries" in the skin to force it to heal. They can be effective but involve "downtime" and can be painful.
Photobiomodulation (PBM): This is often called "Cold Laser" or Low-Level Laser Therapy (LLLT). It does not use heat. Instead of injuring the tissue to trigger a response, it simply feeds the cells the energy (photons) they need to reduce inflammation and repair themselves.
The takeaway: PBM is non-invasive, painless, and has no downtime. It’s "cellular fuel," not a "cellular burn.
Can I use a red light therapy panel for lichen sclerosus?
Many people buy a large wall panel thinking "more light is better," but for VLS, a panel is almost entirely ineffective. Here is the science of why:
The Inverse Square Law (Distance Matters)
In physics, the intensity of light drops off dramatically the further you are from the source. With a panel, you are usually sitting several inches or even feet away. By the time that light reaches your skin, the power density (irradiance) has plummeted. For VLS, we need a high enough "dose" to trigger cellular change, which a distant panel simply cannot provide.
Anatomical Shadowing and Scatter
The vulva is not a flat surface. It has folds, curves, recessed areas, and is tucked away anatomically.
The Shadow Effect: Light from a panel travels in a straight line. It cannot "curve" into the folds of the labia or reach the clitoral hood effectively.
Light Scattering: When light travels through the air from a panel, it hits dust and air molecules, scattering the photons. When you use a contact device (like a handheld laser or a specialized wand), the photons are delivered directly into the tissue without losing energy to the environment.
Tissue Compression
Clinical PBM often uses the "contact technique." By pressing the device gently against the skin, you temporarily displace blood and compress the tissue, allowing the light to penetrate deeper into the layers affected by Lichen Sclerosus. You can't do this with a panel (we do it very very gently with the Solasta laser).
Are there side effects to red light therapy for vulvar skin?
No. This is one of the most common concerns, and it’s important to distinguish PBM from "thermal" or surgical lasers. PBM is often called "cold laser" because it does not produce heat. There is no burning, no cutting, and no trauma to the skin. It is a gentle, biostimulating light that encourages your cells to heal themselves. Most women feel a gentle warmth as blood flow to the area starts to improve. I start with very conservative dosing so as not to aggravate already sensitive tissues and you’ll track your progress along the way.
How soon will I start to feel a difference?
While everyone’s body responds differently, many women in clinical settings report a reduction in itching and "stinging" sensations within the first 3 to 4 sessions. However, for deeper tissue repair and long-term relief, a consistent protocol (usually 10 sessions over several weeks) is recommended to feel the full benefit.
Can I use red light therapy alongside my steroid creams?
Yes. PBM is highly complementary. Many women use it as a supportive tool to help heal the skin while continuing their prescribed steroid regimen. Over time, as the inflammation stays under control and the skin becomes more resilient, some women find they can reduce their reliance on steroids, but you should always coordinate those changes with your specialist.
Why is the specific wavelength of light so important?
Not all "red lights" are created equal. For LS, we look for specific wavelengths that can penetrate the skin effectively. Red light (around 630nm - 660 nm) is excellent for surface-level healing, while Near-Infrared light (around 808 nm) reaches deeper tissues where chronic inflammation lives. Using the wrong wavelength is like trying to tune into a radio station with the wrong frequency - you won't get the "signal" or the results you need.
What about vaginal wands?
As this issue impacts the vulva and usually not inside the vaginal canal I prefer to use a tool I know can deliver the correct amount of energy especially when treating sensitive tissues with LS. My Solasta laser fulfills those requirements. I am a big fan of the Fringe Wand for lubrication, atrophy and collagen improvements and it includes blue wavelengths that can be turned on or off based on how you are tolerating it. I tend to see more noticeable improvements in clients using my Solasta laser than the Fringe wand.
Is PBM a permanent cure for Lichen Sclerosus?
Currently, there is no known permanent cure for LS. However, PBM is a powerful management tool. Think of it like a "rechargeable battery" for your skin’s health. While it can lead to long periods of being symptom-free, most researchers and clinicians recommend occasional "maintenance" sessions to keep inflammation at bay and prevent future flare-ups.
Tracy
Resources:
2024 Study - Journal of Obstetrics and Gynecology
https://www.tandfonline.com/doi/full/10.1080/01443615.2024.2349965#abstract
2017 - Brazil - https://pmc.ncbi.nlm.nih.gov/articles/PMC5550930/
https://doaj.org/article/a272603d01a54d37898e50a490eb6386
Disclaimer: This content is for educational purposes and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your specialist before changing your treatment protocol.