Tired of "Everything is Normal"? NeoFertility Austin Explores Deeper
When “Everything Is Normal” Still Ends in Heartbreak: What the New ASRM Guidelines Mean – and How NeoFertility Goes Further
If you’ve walked through the pain of one miscarriage, you know it changes everything. When it happens again, and especially when it happens more than twice, you start asking deeper questions: Is something being missed? Is there more we can do?
The latest 2026 position paper from the American Society for Reproductive Medicine (ASRM) on recurrent pregnancy loss is a step in the right direction, because it finally says out loud what many couples have felt for years: two losses are enough to deserve a full evaluation. ASRM admits that standard testing often leaves couples with the frustrating label of 'unexplained.' But 'unexplained' often means 'unexplored.' Most traditional clinics check off a basic list and stop there, leaving the root cause hidden.
(Why Didn’t My Perfect Embryo Stick?)
At NeoFertility, that’s where the work really begins. The approach here is multifactorial and clinically driven, built on more than 20 years of hands‑on care by Dr. Phil Boyle and his team, and grounded in careful investigations from cycle to cycle.
First, a quick look at the new ASRM paper
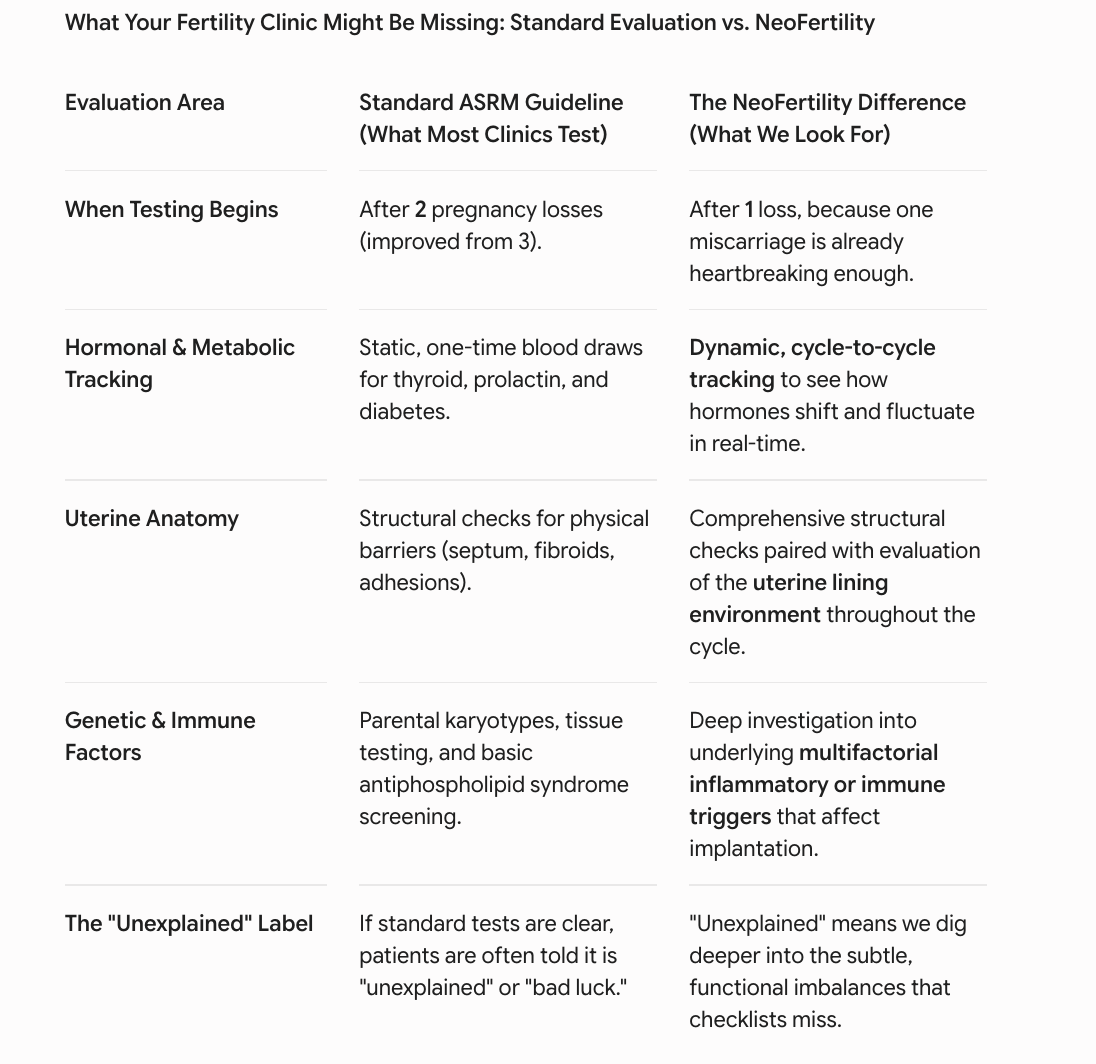
ASRM’s 2026 committee opinion on recurrent pregnancy loss does three key things:
· It defines recurrent pregnancy loss as two or more pregnancy losses, including early “chemical” pregnancies confirmed only by a positive hCG.
· It recommends starting a workup after two losses, not three.
· It focuses evaluation on the areas with the strongest traditional evidence:
o Genetic factors (parental karyotypes, testing of pregnancy tissue where possible)
o Uterine anatomy (looking for septum, fibroids, adhesions)
o Antiphospholipid syndrome
o Key hormonal and metabolic conditions like thyroid disease, prolactin issues, and diabetes
This is the standard, guideline-based foundation and NeoFertility also includes it. However, if your previous clinic told you 'everything looks normal' based strictly on these basic baselines, they likely missed the deeper picture. True answers require looking beyond static checklists.
If you’ve lived through multiple losses, “unexplained” just isnt’ good enough.
The NeoFertility lens: multifactorial, medically led, and based on investigations
NeoFertility uses an approach called Restorative Reproductive Medicine (RRM). It starts with the same foundation ASRM recommends, and then asks a different question:
If the standard tests are normal, what else within the body’s own system might be contributing to these losses?
Rather than assuming there is only one cause, RRM assumes miscarriage is often multifactorial. That means several smaller issues, each one “mild” on its own, can add up to a big impact on whether a pregnancy continues.
Here’s how that plays out in practice at NeoFertility:
· Detailed cycle charting
You learn to chart your cycle carefully - bleeding, cervical mucus, sometimes temperature or urinary hormones - so ovulation is identified precisely, not guessed at. This gives us a real‑time view of how your body is functioning, cycle by cycle.
· Timed mid‑luteal testing (P7 bloods)
Instead of a single “day‑21” progesterone, NeoFertility times blood tests to about 7 days after your ovulation (P7). They look for optimal, not just “in range,” levels
· A broader but focused workup
Depending on your history, additional investigations can include:
o DHEA, DHEA‑S, and testosterone levels.
o Signs of poor follicle function or short luteal phase.
o Investigation of mid-luteal spotting or brown menstrual bleeding.
o Insulin resistance.
o Subtle thyroid or vitamin deficiencies.
o Targeted immune testing (such as NK‑cell panels) when the pattern suggests an immune role.
This is medicine in the classic sense: symptoms, signs, investigations, diagnoses, and then treatments chosen to correct what’s actually found.
From“All your tests are normal” to a healthy baby
A story that will sound familiar to many couples and just one of many in Dr. Boyle’s care at NeoFertility .
A 34‑year‑old woman had:
· Five early miscarriages at around 7 weeks
· Four years trying to conceive
· Normal thrombophilia screen, normal parental karyotypes, normal thyroid function, normal ovarian ultrasound
She then did exactly what ASRM would recommend: she tried another pregnancy with folic acid, low‑dose aspirin, heparin, and progesterone support. That pregnancy also miscarried at 7 weeks…
From a guideline perspective, there was nothing more to offer beyond supportive care. From a NeoFertility perspective, this was the starting point, not the finish line.
NeoFertility investigations uncovered:
· Low DHEA (a key androgen precursor)
· Mildly low endorphin symptoms
· Clinical thyroid dysfunction
· Poor follicle function on P7 bloods
· Brown menstrual bleeding suggesting possible endometritis
Those were treated in a coordinated, multifactorial way: DHEA (once low levels were confirmed), gentle ovarian stimulation, luteal support, antibiotics for suspected endometritis, thyroid support, lifestyle changes, and more. After several cycles of optimizing her health and cycle, she conceived and later delivered a healthy baby boy.
That’s not random experimentation. It’s a structured, investigative process applied over time.
“Is this experimental?” – an important clarification
When you see a plan that includes DHEA, low‑dose naltrexone, timed hCG shots, extra luteal support, or more intensive hormone monitoring, it’s natural to wonder whether this is experimental or standard care.
Here’s what’s important to know:
· This is not a new, untested idea.
Dr. Boyle’s clinical work describes the use of DHEA for preconception optimisation since 2014. This is long‑standing clinical care, refined over thousands of cycles, not a brand‑new protocol being tried for the first time.
· The approach is multifactorial and clinically driven.
Treatments are chosen in response to actual findings - low DHEA on a blood test, poor P7 progesterone, charted signs of follicle dysfunction, evidence of possible endometritis, or immune markers - not given blindly.
· There is published research behind key elements.
A NeoFertility retrospective cohort showed that in pregnancies with low estradiol, supplementing with DHEA (as part of a multifactorial protocol) increased estradiol levels and reduced miscarriage from 45.5% to 17.5% in that high‑risk group. A 2024 case report above shows successful pregnancy after five losses by diagnosing and treating hypoandrogenemia pre‑conception and maintaining DHEA‑guided estradiol levels in pregnancy.
· Off‑label does not mean unsafe.
“Off‑label” simply means a medication is being used in a way that isn’t spelled out on the manufacturer’s package insert, not that it’s unstudied or harmful. In the NeoFertility material, DHEA is described as a naturally occurring hormone precursor that is used to normalize hormone levels, not to push them into extreme ranges. The published work specifically contrasts DHEA with truly harmful drugs in pregnancy and reports healthy birth outcomes when the protocol is followed.
The bottom line: treatments are chosen because they have been observed over many years to improve cycle parameters and pregnancy outcomes in similar patients, and of course medications are are not used when shown to be harmful in pregnancy.
ASRM guidelines + NeoFertility: not either - or
You do not have to choose between “standard guidelines” and NeoFertility. In fact, the most powerful pathway often looks like this:
1. Complete the ASRM‑recommended evaluation
Make sure genetic, uterine, antiphospholipid, thyroid, and metabolic causes have been assessed and appropriately treated.
2. If everything is “normal” but losses continue, move deeper
That is where NeoFertility’s multifactorial, investigation‑based care comes in - looking at cycle patterns, P7 hormone levels, DHEA, thyroid fine‑tuning, insulin resistance, possible immune factors, and more.
3. Build a personalized plan, step by step
Every medication and intervention is tied back to a finding. You see the logic, you see the test results, and you see how each change is designed to restore your own reproductive physiology rather than bypass it.
Why Traditional Clinics Stop Short (And What We Do Differently)
If you are an Austin-area woman who has experienced the heartbreak of recurrent loss, you may have already had some of the ASRM-recommended tests done. If you were told they were "normal," it's incredibly frustrating and I’m sorry you haven’t been offered more investigations.
The truth is, standard fertility clinics typically look at your health on a single day of your cycle. At NeoFertility, we know that pregnancy doesn't happen on a single day. Our approach is cycle-to-cycle and multifactorial. We track, evaluate, and treat the delicate hormonal shifts and underlying conditions throughout your entire cycle to find the subtle imbalances other clinics miss.
Tracy
Recurring Miscarriage - Q&A
Q: My doctor said everything came back "normal" after my miscarriages. How can I still be losing pregnancies?
A: When a standard clinic says your results are "normal," it usually just means your numbers fit into a broad, generic baseline on the specific day your blood was drawn. Pregnancy relies on a continuous, delicate sequence of biological events. A single, static snapshot cannot tell the whole story. At NeoFertility Austin, we evaluate your health dynamically from cycle to cycle to find the subtle imbalances that standard checklists overlook.
Q: What do the new 2026 ASRM guidelines mean for me?
A: The American Society for Reproductive Medicine (ASRM) officially recognized that couples shouldn't have to endure three miscarriages before getting help. The guidelines now state that two pregnancy losses warrant a full evaluation, including early "chemical" pregnancies. This is a massive step forward for patient validation, but it is still just the baseline foundation of care.
Q: Does NeoFertility follow the new ASRM guidelines?
A: Yes, we completely incorporate the standard ASRM recommendations (checking for genetic factors, uterine anatomy, and major hormonal or metabolic conditions). However, we treat ASRM as our starting point, not our finish line. If those standard tests come back normal, our real investigative work begins.
Q: How is the NeoFertility approach different from a traditional IVF clinic?
A: Traditional clinics often use IVF to try and bypass fertility issues. NeoFertility is clinically driven and focused on restorative reproductive medicine. Instead of bypassing the problem, Dr Boyle has spent over 20 years figuring out why the losses are happening. We track your unique cycle to optimize your natural fertility, heal the root cause, and help you sustain a healthy pregnancy.
Resources:
https://www.sciencedirect.com/science/article/abs/pii/S0015028226001275
https://www.asrm.org/practice-guidance/practice-committee-documents/
https://pubmed.ncbi.nlm.nih.gov/42062119/
https://pmc.ncbi.nlm.nih.gov/articles/PMC9213097/