Red Light Therapy for Male Fertility: Is it Safe?
Is red light therapy for male fertility safe? Yes. Clinical reviews show that low-level laser therapy (LLLT) and photobiomodulation are safe and effective for improving sperm motility and reducing oxidative stress. However, success depends entirely on using the correct wavelengths, correct placement, and a low, targeted dose. (Spoiler alert - this is a cold laser - non thermal).
Getting a worrying semen analysis back with low motility or high DNA fragmentation, can feel like you are carrying a problem nobody prepared you for. Male factor infertility contributes to about half of infertility cases, and a meaningful share of male factor cases can also point to underlying health issues that deserve proper workup, not just a quick handoff to IVF or ICSI.
That is why photobiomodulation, also called red light therapy is getting so much attention. The latest review literature finds that most studies using red and near-infrared light report improved sperm motility, and the strongest signal so far is around carefully dosed, targeted treatment rather than generic whole-body light exposure.
What is Photobiomodulation (Red Light Therapy) for Male Infertility
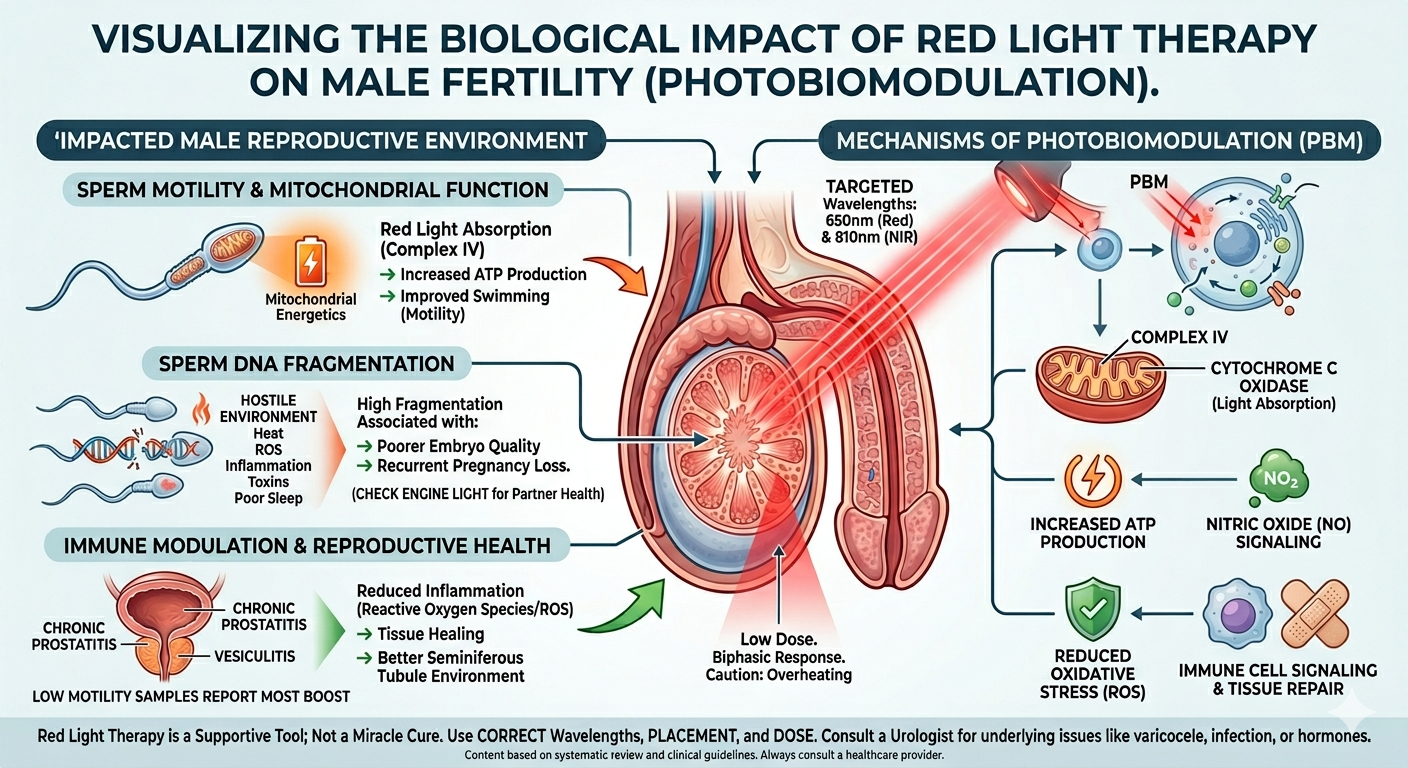
Photobiomodulation uses low-dose red and near-infrared light to support how cells make energy, regulate oxidative stress, and respond to inflammation. In fertility terms, that matters because sperm are especially vulnerable to oxidative stress, mitochondrial dysfunction, and inflammatory damage, all of which can show up as sluggish movement, poor morphology, or elevated DNA fragmentation.
The encouraging part is that red light therapy is not about forcing the body. It is about giving the reproductive system a gentle nudge, especially the mitochondria, circulation, and immune signaling pathways that influence how sperm are made and how well they function.
Red Light Therapy for Sperm Motility and DNA Fragmentation
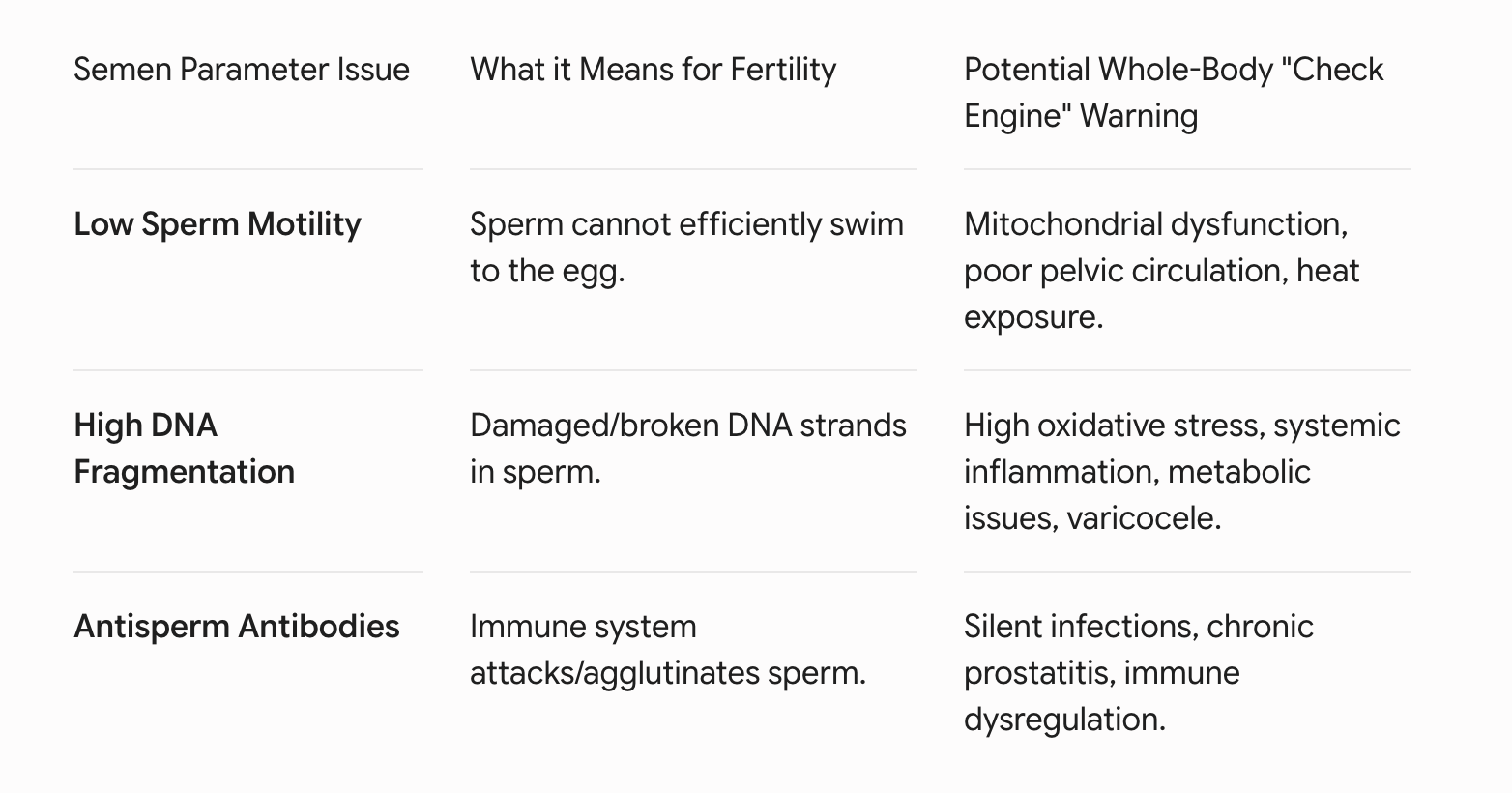
Low motility means sperm are not swimming efficiently enough to make the journey they are designed to make. That can reduce the odds of natural conception and can also be a clue that there is oxidative stress, inflammation, heat exposure, varicocele, hormonal imbalance, toxin exposure, or mitochondrial dysfunction sitting underneath the lab result.
This is where LLLT gets interesting. Human in vitro studies summarized in recent literature show that targeted red and near-infrared light can improve progressive motility and total motile sperm count, especially in low-motility samples, when the dose is low and the wavelength is appropriate. The 2024 systematic review covering studies from 2003 to 2023 concluded that most included PBM studies reported positive effects on sperm motility across red and near-infrared wavelengths.
What high DNA fragmentation can mean
High DNA fragmentation means a larger proportion of sperm carry damaged or broken DNA strands. Clinically, that can be associated with lower natural conception rates, poorer embryo development, recurrent pregnancy loss, failed IVF or ICSI cycles, and a higher level of oxidative stress or inflammation in the male reproductive tract (this is NOT a good sign for your partner’s long-term health).
It does not always mean there is one dramatic diagnosis, but it is often a signal that the sperm are being exposed to a hostile environment. That hostile environment can include excessive reactive oxygen species, unresolved infection or inflammation, heat, metabolic dysfunction, smoking, environmental toxins, poor sleep, and sometimes varicocele or systemic immune dysregulation.
A hostile reproductive environment can include:
Excessive reactive oxygen species (ROS).
Unresolved infections or chronic inflammation (e.g., prostatitis).
Excessive scrotal heat exposure.
Metabolic dysfunction and poor sleep architecture.
How LLLT may help low motility and DNA fragmentation
This is the part that matters most: LLLT may help because it does more than temporarily “wake up” sperm. Photobiomodulation has been shown to influence ATP production, nitric oxide signaling, oxidative stress pathways, tissue healing, and inflammatory regulation, which are all relevant when sperm quality is being undermined by chronic inflammation or oxidative stress.

Solasta Home Laser (includes male factor photobiomodulation protocol).
The immune connection
One of the most overlooked pieces of fertility care is immune modulation. PBM is already studied more broadly for its ability to reduce inflammation, regulate reactive oxygen species, and influence cell signaling involved in tissue repair and immune response. In the male reproductive system, that can matter when inflammatory signaling is contributing to oxidative injury, damage to the seminiferous tubules, or dysfunction in the testicular environment that supports sperm development. In other words, when there is high DNA fragmentation and low motility, the issue is often not that the sperm are “lazy.” The issue is that they are being produced or stored in a biologic environment that is too inflamed, too oxidatively stressed, or too metabolically depleted for optimal function, and LLLT may help modulate that environment in a favorable direction.
Why targeted treatment matters
This is where many people go wrong. More light is not better. The literature repeatedly points to a biphasic dose response - known as Arndt-Schulz Law or the biphasic dose-response curve, meaning too little light yields no effect, an optimal dose stimulates cellular tissue, and an excessive dose inhibits function or causes thermal damage which means the right amount may help, but too much may flatten the benefit or work against the outcome you want. That is also why targeted, low-dose protocols make more sense than simply standing in front of a red light panel and hoping for the best. We’re looking for the ‘goldilocks’ zone.
Why advanced male testing can get skipped in IVF settings
In some IVF settings, advanced male factor tests such as sperm DNA fragmentation or antisperm antibody testing are not performed routinely before moving to ICSI. That is not necessarily poor practice, because major guidelines do not recommend either test in the initial evaluation of every infertile couple; sperm DNA fragmentation testing is usually reserved for selected situations such as recurrent pregnancy loss, varicocele, prior ART failure, or other scenarios where the result could change management, and antisperm antibody testing is generally considered only when history or semen findings suggest it may be relevant.
At the same time, it is clinically fair to say that ICSI can bypass some barriers without fully addressing the upstream male biologic environment. ICSI solves a mechanical problem by placing a single sperm directly into the egg, so it can overcome poor motility and can also bypass the functional effect of antisperm antibodies on sperm transport or sperm-egg interaction, but it does not automatically correct oxidative stress, inflammation, infection, varicocele-related damage, or abnormal sperm DNA integrity in your partner.
Sometimes the clinical pathway moves quickly to ICSI because it is an efficient laboratory workaround for male factor infertility, but that does not mean the underlying contributors to sperm injury have been fully investigated. If a man has high DNA fragmentation or evidence of an inflamed reproductive environment, the concern is not that ICSI is “wrong”; the concern is that a sperm selected for injection may still come from a biologic setting marked by oxidative stress or inflammation, which can be associated with poorer embryo development and, in some studies, higher miscarriage risk.
Male fertility as a “check engine light” for overall health
When a semen analysis comes back with low count, low motility, or high DNA fragmentation, it is easy to see it as a problem that lives only in the fertility clinic. But the research paints a different picture. Large studies now show that male factor infertility is often a window into your partner’s overall health, not just a barrier on the road to pregnancy.
Men with abnormal semen parameters are more likely to have underlying cardiometabolic issues like insulin resistance, diabetes, high blood pressure, and obesity, even when they feel “fine” day to day. They also carry a higher risk of certain cancers (especially testicular and prostate cancer) and, in more severe cases such as azoospermia, a higher risk of long-term health problems and earlier mortality compared with fertile men of the same age.
A concerning semen analysis is not just bad news; it is valuable information. It means we need to zoom out and ask the bigger question, “What is this telling us about whole-body health, inflammation, hormones, and lifestyle?” rather than just, “How fast can we get to ICSI?” That is exactly where tools like targeted LLLT, nutrition, sleep, movement, and proper medical workup all work together - supporting both fertility and long-term health at the same time. This where the approach of NeoFertility and Restorative Reproductive Medicine shines.
Where antisperm antibodies fit in
Antisperm antibodies are not the most common driver of infertility, and many men with detectable antibodies do not have clinically meaningful fertility problems. However, when they are significant, they can impair motility, cause sperm agglutination, and interfere with normal sperm transport or sperm-egg interaction, which is one reason ICSI is often effective in these cases.If a clinic goes straight to ICSI, it may successfully bypass the motility or binding problem caused by antisperm antibodies, but it still may not answer the bigger question of why the antibodies or inflammatory signals are present in the first place. That broader question can matter when there are repeated failed cycles, poor embryo quality, elevated leukocytes, recurrent pregnancy loss, or semen patterns that suggest a deeper inflammatory issue or silent infection.
What is the body trying to tell us?
If a semen analysis shows low motility or high DNA fragmentation, that result is not just a number to work around. It is information. It may be a clue that the male reproductive environment needs support at the level of oxidative stress, mitochondrial function, immune balance, circulation, or all four at once. That is what makes LLLT so compelling. It is not a promise. It is not a substitute for seeing a urologist, evaluating varicocele, infection, hormones, medications, and lifestyle exposures, or repeating a semen analysis after a full sperm cycle of about 74 days. But it is a science-backed tool that may help support motility, reduce oxidative challenges, and improve the environment in which sperm are produced and mature.
We’ve been trying for 6 months and we’re not pregnant yet — can we both use the Solasta laser now?
If you have been trying for 6 months and you are not pregnant yet, it is completely reasonable to pause and ask bigger questions, especially if the female partner is 35 or older or if either partner has known risk factors. Clinical guidance usually advises evaluation after 12 months for couples under 35, but after 6 months when the female partner is 35 or older, and earlier when there are red flags like irregular cycles, prior pelvic disease, varicocele, infections, or a history that suggests male factor may be in play.
And here is the important part: yes, it can make sense to support both partners, even before you have a confirmed male factor diagnosis, because fertility is a shared biologic process and male issues are often silent. Many men with low motility, high DNA fragmentation, prostatitis, oxidative stress, or early inflammatory changes have no obvious symptoms at all, which is one reason male factor so often gets missed until couples are already further down the fertility path.
For men especially, there can be “quiet” contributors sitting in the background, including low-grade inflammation, silent infections, prostatitis, vesiculitis, oxidative stress, heat exposure, or poor pelvic circulation. Chronic prostatitis and inflammatory conditions of the male reproductive tract have been associated with poorer semen quality, and older laser therapy research reports that low-level laser therapy used in men with prostatitis and vesiculitis improved inflammatory changes and was associated with better sperm motility and reproductive function. This has also been my experience with couples using my laser at home.
That does not mean LLLT replaces proper testing or antibiotics when infection is present. A clinically correct way to say it is that LLLT may be a useful supportive therapy because it can help modulate inflammation, improve circulation, support tissue repair, and reduce oxidative stress, all of which may matter when an inflamed reproductive environment is interfering with sperm quality.
So if you are six months in and still not seeing a positive test, the next step does not have to be panic. It can be a smarter, more supportive plan: evaluate both partners, look for the silent stuff, and use tools like targeted LLLT to support the biologic environment while you are getting clearer answers.
You do not need to wait for a dramatic diagnosis to start supporting fertility. Sometimes the most powerful move is to care for both bodies early, especially when male factor issues can be present long before they are obvious on paper.
Because no two male fertility cases look exactly the same, I also write personalized protocols for partners who are using my Solasta laser, including targeted laser guidance, lifestyle support, supplement strategy, and next-step testing questions, so you are not left trying to piece it all together on your own.
Frequently Asked Questions
Is red light therapy safe for sperm and testicles?
Yes, red light therapy - scientifically known as photobiomodulation (PBM) is safe for sperm when applied using the correct wavelengths and a low, controlled dose. Because the testicles are highly sensitive to temperature, the therapy must remain strictly non-thermal. Utilizing low-level, high-quality devices that do not emit ambient heat ensures the tissue stimulates cellular energy without overheating the delicate environment where sperm are produced.
Can red light therapy improve low sperm motility?
Yes. Clinical studies show that targeted red and near-infrared light absorbed by the sperm’s mitochondria increases the production of Adenosine Triphosphate (ATP), which acts as the cellular fuel. This boost in cellular energy directly enhances progressive motility and total motile sperm count, giving sluggish sperm the energy required to swim more efficiently.
How does photobiomodulation help with high sperm DNA fragmentation?
High DNA fragmentation is often driven by an inflamed, oxidatively stressed reproductive environment. Photobiomodulation works upstream by downregulating chronic inflammatory pathways, regulating reactive oxygen species (ROS), and improving local pelvic circulation. By modulating the biological environment where sperm mature, it shields developing cells from oxidative damage.
What wavelengths of light are best for male fertility?
The peer-reviewed literature demonstrates that the most effective wavelengths sit within the optical window of 650nm (visible red light) and 810nm to 850nm (near-infrared light). These specific wavelengths are absorbed by an enzyme in the mitochondria called cytochrome c oxidase, triggering the beneficial cellular cascade without generating dangerous tissue heating.
Why is a whole-body red light panel not recommended for testicular health?
More light is not better due to the biphasic dose-response curve (the Arndt-Schulz Law). While an optimal, localized low dose stimulates cellular health, an excessive or prolonged dose from a large, high-powered whole-body panel can flatten the therapeutic benefit or cause thermal stress to the testicles. Targeted, precise dosing is critical for reproductive success.
How long does it take to see improvements in a semen analysis?
Because human spermatogenesis (the timeline for the body to produce and mature a new cycle of sperm) takes approximately 74 days, any supportive therapy, including red light therapy, targeted supplementation, and lifestyle changes, should be maintained consistently for at least 2.5 to 3 months before repeating a semen analysis to accurately evaluate progress.
Can red light therapy replace ICSI or IVF for male factor infertility?
Photobiomodulation is a supportive, restorative therapy rather than a mechanical workaround. While treatments like Intracytoplasmic Sperm Injection (ICSI) solve the mechanical challenge of fertilizing an egg with sluggish sperm, they do not correct underlying cellular issues like oxidative stress or inflammation. Red light therapy works to improve the actual biological quality of the sperm being used, whether attempting natural conception or preparing for an upcoming IVF/ICSI cycle.
Tracy
References & Further Reading
https://blog.tracydonegan.org/blog/is-testosterone-therapy-harming-your-chances-of-conceiving
Systematic Review (2003–2023): Moradi, S., et al. A Comprehensive Systematic Review of the Effects of Photobiomodulation Therapy on Sperm Cell Characteristics. Reproductive Sciences, 2024.
Clinical Guidelines: Diagnosis and Treatment of Infertility in Men: AUA/ASRM Guideline Part I. American Society for Reproductive Medicine, 2020.
Mitochondrial Study: Balbi, M., et al. Efficacy and Safety of Visible and Near-Infrared Photobiomodulation Therapy on Asthenozoospermic Human Sperm. Biology, 2025.
Prostatitis and LLLT: Low-Level Laser Therapy in Chronic Prostatitis and Vesiculitis Management. Urologia, 2002.
Antisperm Antibodies Data: Antisperm Antibodies and Male Fertility: New Insights From a 10-Year Study. MES Global Insights.
This education is designed to support informed decision-making and is not a substitute for individualized medical diagnosis or treatment.