The Shadow Costs of IVF: What You Don’t Know Can Hurt You - and Your Baby
The Shadow Costs of IVF: What Most Women Aren’t Told About the Price of Getting Pregnant
Most women do not walk into a fertility clinic saying, “What I really want is IVF.” They walk in saying, “I just want a baby.” That longing is real, and often urgent. In that vulnerable place, IVF can sound like the clearest, fastest, most hopeful answer available.
And sometimes IVF truly is an appropriate next step. But in 2026, the conversation needs to be more transparent and more informed. Fertility benefits like Carrot and other employer-sponsored programs have made IVF more financially accessible for many families, but access is not the same thing as informed consent. A benefit can lower the upfront bill, yet still leave women unaware of the physical costs, the emotional costs, and the downstream medical costs that can follow an IVF pregnancy.
That is where the shadow costs come in.
The visible cost is only part of the story
When IVF is discussed, the headline number is usually the clinic quote. In the United States, one IVF cycle with medications and common add-ons is often framed as roughly $20K to $30K depending on medications, monitoring, frozen transfer plans, and genetic testing. In 2026, TrumpRx has made some IVF medications more affordable for qualifying self-pay patients through discounted pricing on selected EMD Serono drugs, with federal and clinic sources describing savings of about $2,000 to $2,200 per cycle on average for those who use the covered medications together. Even with that improvement, employer fertility benefits and drug discounts often use dollar caps, limited formularies, or medication-specific eligibility rules, which means many couples still face meaningful costs and the benefit may only fully fund one cycle, not the multiple cycles many eventually need.
That matters because IVF is usually priced per cycle, but lived emotionally and financially across multiple attempts. Many couples do not get a baby from one retrieval and one transfer. They may need additional stimulation cycles, frozen embryo transfers, more medication, more time off work, more travel, and more emotional recovery between rounds.
So yes, fertility benefits and TrumpRx are changing the cost conversation in a real way. Lower medication prices are genuinely helpful, and that is good news for patients. But they are not making IVF free. TrumpRx currently applies to only certain fertility drugs, not every medication used in an IVF protocol, and some pharmacies may add separate dispensing, shipping, coordination, or service fees that affect the final bill. On top of that, insurance design can still leave deductibles, coinsurance, uncovered add-ons, and the quiet financial strain that comes with a longer-than-expected fertility journey.
Insurance can pay a bill, but it cannot change biology
This is the part many women never hear clearly enough: fertility benefits reduce financial friction, but they do not erase medical risk. Even in the era of better embryo selection and more single embryo transfer, IVF singleton pregnancies still show higher risks of preterm birth and NICU admission compared with spontaneously conceived single babies.
That distinction matters because most women are understandably focused on one thing: getting pregnant. But the true goal isn’t simply a positive test. The more important goal is a healthy pregnancy, a full-term baby, and a family that is not blindsided by often preventable complications.
Restorative Reproductive Medicine, or RRM, starts from that broader goal. Instead of bypassing the cycle, RRM asks why your cycle is not working well in the first place and works to restore ovulation quality, hormone balance, cervical mucus, thyroid function, metabolic health, male factor contributors, and other root causes of infertility.
Who often comes to NeoFertility in the first place?
A crucial piece of context is that many NeoFertility and broader RRM patients are not uncomplicated, first-step fertility patients. They often arrive after years of infertility, prior miscarriages, prior surgeries, hormone dysfunction, thyroid or metabolic issues, suspected endometriosis, male-factor challenges, or one or more failed IVF attempts.
In one of the best-known published RRM cohorts after failed IVF, 403 couples had already undergone an average of 2.1 prior IVF attempts and had been trying to conceive for an average of 5.8 years. The average female age was 37.2, and only 5% had previously taken home a baby from IVF, which makes this a medically and emotionally complex group rather than an easy-prognosis population.
That matters because it reframes the comparison. NeoFertility is often not seeing women at the beginning of the road. It is often caring for women and partners who have already been through the fertility system, have already spent money, and still have underlying health patterns that were never fully worked up or corrected before another embryo transfer was attempted.
This is why restorative care puts investigation first. If a woman has inflammation, poor ovulation, low progesterone, thyroid dysfunction, insulin resistance, endometriosis, recurrent miscarriage, poor cervical mucus, chronic infection, or a male-factor issue, those are not side notes. They are part of the fertility story and part of the pregnancy-risk story. NeoFertility’s model is to treat those first, not as an optional extra, but as the foundation for a healthier conception and pregnancy.
IVF pregnancies can be higher risk for women too
Large studies and reviews show that pregnancies conceived with IVF have higher rates of certain maternal complications than pregnancies conceived spontaneously, even after adjusting for some risk factors.
Those complications can include pregnancy-induced hypertension, gestational diabetes, placental problems, cesarean delivery, postpartum hemorrhage, and severe maternal morbidity. One large cohort found severe maternal morbidity was markedly more common after IVF than after natural conception, even in women otherwise considered low risk.
This is an important point for women who are told to think only about getting pregnant as quickly as possible. A positive test is not the whole story. Your health during your pregnancy and birth matters too. I know it’s really hard to think past just getting that long awaited positive pregnancy test but there are other ways to get you to there than reduce all of these risks. Getting you as healthy as possible and addressing any underlying health conditions NOW and not when you’re pregnant and you have a growing baby to think about too.
What happens to your birth options after IVF?
If you conceived through IVF, there’s something most women are never told and it breaks my heart as a midwife: the minute “IVF” lands on your chart, many systems stop seeing you as a low‑risk pregnant woman and start seeing you as high‑risk by default.
Because large population studies show higher rates of complications and cesareans in IVF pregnancies, many hospitals and group practices write policies that automatically funnel IVF moms into obstetric‑managed, high‑risk pathways, even when your pregnancy itself is going perfectly. That can quietly close the door to midwifery‑led options (you’ve been dreaming about a waterbirth…not in an Austin area hospital). If you’ve been taking GLP-1s before becoming pregnant your risk of several pregnancy complications can increase quite significantly. If you’ve been recommended these medications by your clinic/OB I hope they have shared this information with you so you could make an informed decsion about your medications. This is yet another reason why a root cause - restorative approch to fertility matters. We focus on helping you get to optimal health BEFORE conceiving.
In real life, that often looks like this:
You are excluded from midwifery‑only or birth‑center programs that are reserved for “low‑risk” pregnancies, with IVF listed as a disqualifier.
Your primary care is assigned to an obstetrician, sometimes with maternal‑fetal medicine oversight, and you see a midwife in your hospital - they are there as support staff rather not as your primary care provider.
For many IVF moms who want true continuity of midwifery care, the only way to access it is outside the hospital system, through homebirth or very flexible independent midwifery practices.
Even with a perfectly healthy pregnancy, an IVF label changes how your labor is managed. Studies consistently show that IVF pregnancies have higher rates of induction and cesarean than spontaneous conceptions, even for single babies born at term. Part of that is medical (older age, twins, placenta issues), but part of it is culture: after so much emotional and financial investment, clinicians are quicker to induce “just in case,” to keep you on continuous monitoring, and to move to a cesarean if you cough too hard.
None of this means you cannot have a beautiful, empowering birth after IVF. It does mean you deserve to know that:
As an IVF mom, you are more likely to be categorized as high‑risk, even if you feel well. Some women are quite happy with this option.
That high‑risk label often takes midwifery‑led hospital care off the table, unless you choose homebirth or work with a team that is comfortable supporting IVF pregnancies as normal when the evidence allows.
Being cared for primarily by an obstetrician in a high‑intervention setting makes inductions, continuous monitoring, epidurals, assisted births and cesareans statistically more likely, simply because the threshold for intervening is lower.
One of the reasons a restorative approach focuses on correcting root‑cause issues before conception is not just to help you get pregnant, but to give you the best chance of a pregnancy and birth that can be treated as physiologically normal, so that more care models, including midwifery, stay open to you where they’re available.

Home waterbirth with Midwifery Led care
Finding the Root Cause Has Implications for Your Pregnancy and Birth
This is where the conversation becomes more nuanced. Some of the increased risk is related to the very reasons women need IVF in the first place: older age, endometriosis, PMOS, inflammation, uterine factors, thyroid issues, insulin resistance, male factor infertility, or previous reproductive loss.
But the data suggest it is not only the underlying infertility. Studies that try to adjust for infertility diagnoses still find risk differences linked to IVF itself, including effects associated with stimulation, embryo culture, frozen embryo transfer protocols, and endometrial preparation.
So the most honest answer is that both things can be true at once. If you’re already not in peak health your body is already be under strain, and the IVF process may add another layer of stress on top. In plain language, fertilization in the lab does not automatically correct inflammation, poor hormone signaling, endometrial dysfunction, thyroid imbalance, metabolic issues, or other root-cause problems that can still shape placentation, blood pressure, blood sugar, fetal growth, and timing of your baby’s birth.
That is one of the central differences in RRM. Instead of asking, “How do we get an embryo created and transferred as fast as possible?” restorative care asks, “Why is this body struggling to conceive or sustain pregnancy, and what needs to be corrected before or alongside conception?”
Your baby’s risk matters too
Recent studies continue to show that singleton pregnancies conceived by IVF carry a higher risk of preterm birth than spontaneous singleton pregnancies. That does not mean every IVF baby will be born early, and it does not mean parents who choose IVF are doing anything wrong. It simply means the risk profile is different, and families deserve to know that before they make decisions under stress.
The financial side of that risk is significant. U.S. analyses have estimated average NICU spending per admission at roughly $71,000, with severe cases costing far more. Another recent analysis reported median hospitalization costs in the hundreds of thousands of dollars for extremely preterm infants, while even less severe NICU stays can still create major insurance and out-of-pocket burdens for families.
Even when insurance covers much of the hospital bill, the shadow costs remain. New parents can still face deductibles, coinsurance, missed work, childcare for older children, parking, travel, meal costs, and the emotional trauma of watching their baby receive intensive care instead of going home together.
This is an important distinction in the fertility-benefit era: when an employer pays for part of IVF, that may reduce the upfront treatment bill, but it does not protect a family from every downstream consequence of a higher-risk pregnancy.
Success rates matter. But so does what happens after the positive test.
IVF carries meaningful risks beyond the pregnancy attempt itself. The national IVF preterm birth rate is 14.4% and the twin rate sits at around 6% - even as single embryo transfer practices have improved (SART 2023; CDC ART National Summary).
Here in Austin, the picture varies considerably by clinic. These are the 2023 SART figures for women under 35 using their own eggs:
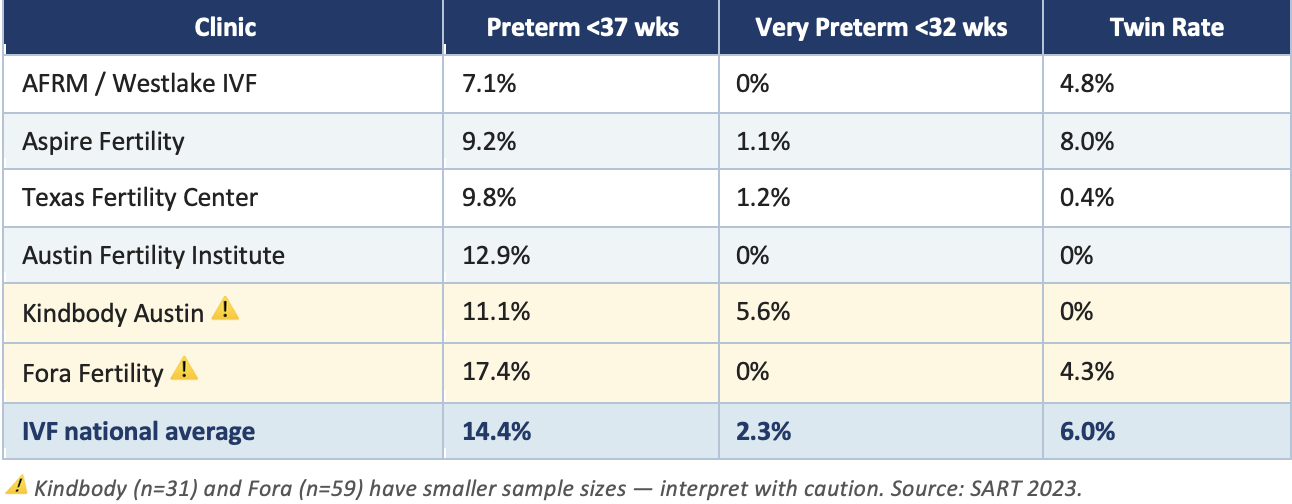
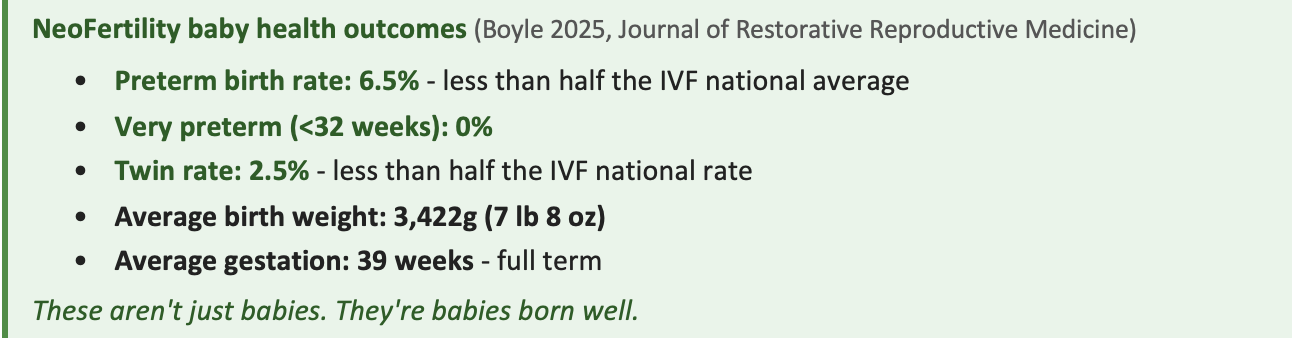
The NeoFertility approach focuses on balancing hormones so you produce ONE healthy follicle. Keeping you and your baby safer.
The additional out-of-pocket costs couples often don’t expect
When women compare IVF and RRM, they often compare the clinic fee and stop there. But there are many possible out-of-pocket costs that can stack up around IVF even when some treatment is covered by insurance or by an employer fertility benefit.
These may include:
· Deductibles and coinsurance for clinic visits, procedures, anesthesia, hospital-based retrievals, ultrasounds, and laboratory services.
· Medication costs that exceed benefit caps or fall outside pharmacy coverage, especially in higher-stimulation protocols; even with TrumpRx, only certain medications are discounted, so many protocols still include uncovered drugs or extra pharmacy-related fees.
· Genetic testing, embryo storage, frozen embryo transfer fees, ICSI, assisted hatching, and other add-ons not always fully covered.
· Travel, hotels, parking, meals, childcare, and missed wages from repeated early-morning monitoring and procedure days.
· Maternal complication costs related to hypertension, cesarean birth, hemorrhage, hospital readmission, or postpartum recovery needs.
· NICU-related family expenses, including high deductibles, coinsurance, transportation, meals, lodging, and unpaid leave if a baby is born early.
Taken together, these shadow costs can make a “covered” IVF journey much more expensive than a family expected when they first heard the words, “Good news, your employer offers fertility benefits.”
Why this changes how the options should be framed
For many women, the real question isn’t “Can I access IVF?” The real question is “What path gives me the best chance of bringing home a healthy baby without taking on avoidable risks and costs along the way?”
That is where RRM deserves a serious place in the conversation. Evidence summarized by RRM-focused organizations and recent commentary on restorative approaches argues that this model can produce healthier outcomes that are meaningful and clinically relevant, especially because it aims for healthier singleton pregnancies rather than simply achieving conception by any means necessary.
One RRM analysis comparing outcomes with IVF reported lower preterm birth and lower twin rates than IVF cohorts, which matters not just medically but economically. In the published post-IVF RRM cohort, the adjusted live birth rate was 32.1% after an average of 2.1 prior failed IVF cycles, with 92% of babies born at 37 weeks or later and only one twin pregnancy in the entire study population. Fewer preterm births can mean fewer NICU stays, fewer emergency expenses, fewer traumatic postpartum experiences, and less long-tail financial stress after the baby arrives.
This is why the comparison cannot be reduced to “Is IVF covered by my employer?” A covered intervention can still carry hidden costs. A less glamorous path can still be the wiser investment if it supports maternal health, reduces prematurity risk, and helps a couple build a family with fewer complications (especially if you would like to have more than one baby).
Compassion first, always
None of this is meant to shame women who choose IVF. Many do so after years of trying, losses, surgeries, low ovarian reserve, male factor infertility, or the kind of heartbreak that makes speed feel like survival. Wanting the fastest path does not make anyone naive. It makes them human.
But women deserve more than marketing. They deserve a conversation that includes the visible cost and the invisible one. They deserve to know that fertility benefits are a gift for many families, but not a full answer. They deserve to understand that paying less out of pocket for IVF is not the same thing as reducing every risk to their baby, their body, or their future finances.
And they deserve to hear that there is another framework available. Restorative Reproductive Medicine asks not only how to achieve pregnancy, but how to restore health in a way that supports conception, implantation, and a healthier full-term birth. For many couples, that question may be the most important one of all.
Most women do not need more pressure.They need clarity.
A compassionate way to frame the conversation is this:
· IVF may be more financially accessible today because of employers, fertility benefits, and newer medication discounts like TrumpRx.
· That does not mean IVF is free, fully covered, or risk-free; drug discounts help, but they do not remove all medication costs, add-on fees, or downstream pregnancy-related expenses.
· The hidden costs may include multiple cycles, medication, time off work, emotional burnout, maternal complications, higher odds of preterm birth, and possible NICU-related expenses.
· Some of the risk comes from the underlying infertility itself, but research suggests IVF can add its own layer of risk rather than removing the root-cause issues that may have contributed to infertility in the first place.
· RRM offers a different path, one focused on identifying and treating the root causes of infertility while supporting healthier pregnancies and lower downstream risk.
Does your employer offer RRM coverage for employees who prefer not to go down the IVF route - or have already had a difficult time with IVF?
Tracy
https://pubmed.ncbi.nlm.nih.gov/38796038/
https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2023.1065291/full
https://pmc.ncbi.nlm.nih.gov/articles/PMC12505749/
https://pmc.ncbi.nlm.nih.gov/articles/PMC6079215/
https://www.frontiersin.org/journals/medicine/articles/10.3389/fmed.2018.00210/full
https://pubmed.ncbi.nlm.nih.gov/30109231/
https://pmc.ncbi.nlm.nih.gov/articles/PMC11980792/
https://pmc.ncbi.nlm.nih.gov/articles/PMC9635605/
https://www.nature.com/articles/s41598-022-08707-x
https://pmc.ncbi.nlm.nih.gov/articles/PMC9773093/
https://www.nature.com/articles/s41372-026-02619-8
https://healthcostinstitute.org/all-hcci-reports/nicu-use-and-spending-1/